

out of how many nuclei does the oculomotor nucleus consits?
what do they supply?
what do they supply?
six,
five somatic subnuclei supply the motor inntervation for 4 of the 6 extraocular muscles that move each eye plus levator palpebrae superioris which elevates the uper eyelid
one medially situated parasympathetic edinger westhhal subnucleus.
five somatic subnuclei supply the motor inntervation for 4 of the 6 extraocular muscles that move each eye plus levator palpebrae superioris which elevates the uper eyelid
one medially situated parasympathetic edinger westhhal subnucleus.
through which foramen exits the oculomotor nerve?
whcih division does it have?
what do they supply?
whcih division does it have?
what do they supply?
superior orbital fissure
upper diviison and lower division
upper division: superior recturs and levator palpebrae superioris
lower division: medial rectus, inferior rectus and inferior oblique
upper diviison and lower division
upper division: superior recturs and levator palpebrae superioris
lower division: medial rectus, inferior rectus and inferior oblique
the oculomotor nerve has a nucleus with parasympathetic nerve fibres. with what do they synapse?
where do they go after they synased?
where do they go after they synased?
ciliary ganglion
postganglionic fibres run in the short ciliary nerves to sclera, pierce the lamina cribrosa and supply the ciliary and sphincter pupillae muscle
postganglionic fibres run in the short ciliary nerves to sclera, pierce the lamina cribrosa and supply the ciliary and sphincter pupillae muscle
what is parital 3rd nerve palsy?
what does it cause
what is it caused by
what does it cause
what is it caused by
parasympathetic fibres become compressed as they are the most superficial ones and are comressed against the petrous part of the temporal bone
causes pupil of affected side to dilate progressivley
may be caused by increased intracranial pressure and sxtra or subrudal ahemtatoma (pupoils shoudl also be monitored in head injury, indicate compression)
causes pupil of affected side to dilate progressivley
may be caused by increased intracranial pressure and sxtra or subrudal ahemtatoma (pupoils shoudl also be monitored in head injury, indicate compression)

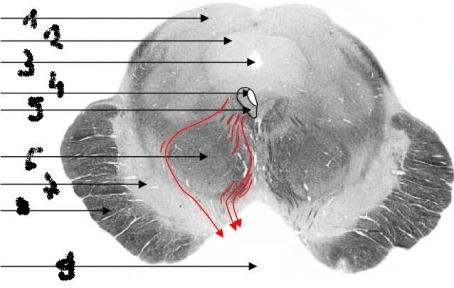
1 trohlear nerve
2 inferior colloculus
3 cerebral aquiduct
4 periaquiductal grey matter
5 trochlear nuclues
6 median longitudional fasciculus
7 desuccation of superior cerebellar peduncles (cerebellar-rubro-thalamic pathway)
8 substantia nighra
9 cerebral peduncle
10 interpeduncular fossa
11 oculomotor nerve
2 inferior colloculus
3 cerebral aquiduct
4 periaquiductal grey matter
5 trochlear nuclues
6 median longitudional fasciculus
7 desuccation of superior cerebellar peduncles (cerebellar-rubro-thalamic pathway)
8 substantia nighra
9 cerebral peduncle
10 interpeduncular fossa
11 oculomotor nerve
what are the symptoms of trochlear nerve palsy?
double vision (down and out diplopia) when looking downwards
torticollis ( coensatory tiliting of the head to the side oposite the palsied ee
eye driting upwards, as superior oblique is paralysed, it normally helps the inferior rectus to pull the eyeball dwonwards in medial position . this is known as hypertropia.
torticollis ( coensatory tiliting of the head to the side oposite the palsied ee
eye driting upwards, as superior oblique is paralysed, it normally helps the inferior rectus to pull the eyeball dwonwards in medial position . this is known as hypertropia.


where does the nuclei of the abducends lie?
through which frissure does it ass?
what msucle does it supply?
through which frissure does it ass?
what msucle does it supply?
lie in the floow of the forth vetnricle at the level of the facial colliculi,
fibres run anteriorly and ipsilaterally though the pons to emerge at the inferior border near the midline
superior orbital frissure
lateral rectus muscles (ABducts)
fibres run anteriorly and ipsilaterally though the pons to emerge at the inferior border near the midline
superior orbital frissure
lateral rectus muscles (ABducts)

what is the tympanic branch? what does it supply?
is sensory to the tympanic cativy where it suppplies the middle ear
affernt fibres project to the spinal trigeminal nucleus
parasympathetic fibres of the tympanic nerve originate form the infeiror salivatory nucles ( part of the nuclei of the CN 9) and continue form the tympnaic plexus in the middle ear as the lesser petrosal nerve (the part of the typmanic nerve that is parasympathetic) to the otic gangion which which postgangionic fibres run in the auriculotemporal nerve (branch of the mandibular nerve v3) to supply the parotid gland.
affernt fibres project to the spinal trigeminal nucleus
parasympathetic fibres of the tympanic nerve originate form the infeiror salivatory nucles ( part of the nuclei of the CN 9) and continue form the tympnaic plexus in the middle ear as the lesser petrosal nerve (the part of the typmanic nerve that is parasympathetic) to the otic gangion which which postgangionic fibres run in the auriculotemporal nerve (branch of the mandibular nerve v3) to supply the parotid gland.
what does the carotid branch of the CN 9 supply?
carries afferent barorepective fibres which originate in the carotid sinus which are sensitive to systoic blood prssure. They procjet to the baroreceptor region of the nuclues solitarous
chemorecetpive fibres which supply the glommus cells ot the carotid body monitoring CO2 and O2 levels and projet to the dorsal resporatory region fo the nucleus solitarius
chemorecetpive fibres which supply the glommus cells ot the carotid body monitoring CO2 and O2 levels and projet to the dorsal resporatory region fo the nucleus solitarius
from whch nucleus does the effernt fibres to the stylopharyngeus arise?
nucleus ambigous (This nucleus gives rise to the somatic efferent motor fibers of the vagus nerve (CN X) terminating in the laryngeal and pharyngeal muscles, as well as to the efferent motor fibers of the glossopharyngeal nerve (CN IX) terminating in the stylopharyngeus)
in the oropharnyx, the CN9 conveys which fibres to where?
afferent fibres
-supply sensation to the posterior thir of the tongue ( gag reflex)
-musouc membrane
-taste fibres of the cicumvallate papillae at the back of the tongue project to the gustatory region o the nucleus solitarious
VISCERAL AND TASTE FIBRES ALL END IN THE NUCLEUS SOLITARIUS
AFFERENT FIBRES OF GENERAL SENSATION END IN THE TRIGEMINAL SENSory NUCELUS
-supply sensation to the posterior thir of the tongue ( gag reflex)
-musouc membrane
-taste fibres of the cicumvallate papillae at the back of the tongue project to the gustatory region o the nucleus solitarious
VISCERAL AND TASTE FIBRES ALL END IN THE NUCLEUS SOLITARIUS
AFFERENT FIBRES OF GENERAL SENSATION END IN THE TRIGEMINAL SENSory NUCELUS
the VN has many branches. we concentrate on two. which are the two important ones? what fibres do they carry?
where do they have their cell bodies?
where to they go to?
where do they have their cell bodies?
where to they go to?
auricular branch
carries cutaneous sensation form the skin lining the external auditory meatus
menigeal branch
carris sensation form the postteror cranial fossa
both have their cell bodies in the jugular ganglion and their central processes project to the spinal trigeminal nucleus.
carries cutaneous sensation form the skin lining the external auditory meatus
menigeal branch
carris sensation form the postteror cranial fossa
both have their cell bodies in the jugular ganglion and their central processes project to the spinal trigeminal nucleus.
where do the special visceral effent fibres arise from the vagus and what do they innervate?
where to the general visceral afferent fibres have their cell body and what do they supply?
where to they habe their cell bodies?
where to they project to ?
where to the general visceral afferent fibres have their cell body and what do they supply?
where to they habe their cell bodies?
where to they project to ?
arise form nucleus ambiguus
form braches the pharyngeala nd the laryngeal of the vagus which supply :
solft palate, larnyx pharyx, levator palatini, upper striated muscles of the oesi
-> imortant for speech and swallowing
form heart and respiratroy and alimentary tracts
inferior nodose gangion
comissural region of the nucleus solitarius
form braches the pharyngeala nd the laryngeal of the vagus which supply :
solft palate, larnyx pharyx, levator palatini, upper striated muscles of the oesi
-> imortant for speech and swallowing
form heart and respiratroy and alimentary tracts
inferior nodose gangion
comissural region of the nucleus solitarius
what type is the spinal acessory nerve, motor or sensory?
where does it derive from?
through which foramen does it exit?
what does it supply?
where does it derive from?
through which foramen does it exit?
what does it supply?
motor
nucleus of the accessory nerve (column af alpa and gamma neurons)
enter the cranium though the foramen magnum and leateit again through the jugular foramen
sternocleidomastoids (alsong with C2 and 3)
trapezius (along with c3 and 4)
nucleus of the accessory nerve (column af alpa and gamma neurons)
enter the cranium though the foramen magnum and leateit again through the jugular foramen
sternocleidomastoids (alsong with C2 and 3)
trapezius (along with c3 and 4)
what kind of fibres does the hypoglossal nerve contain?
what doe they supply?
from waht structres does the hypoglossal nucleus receive fibres from?
through which foramina does it leave the cranium?
what doe they supply?
from waht structres does the hypoglossal nucleus receive fibres from?
through which foramina does it leave the cranium?
somatif efferents
extrnsic and intrinsic muscles fo the tongue
reticular neurons (for automatic of reflex movements in eating of swallowing) and cortical fibres (for speech articulation)
hypoglossal canal
extrnsic and intrinsic muscles fo the tongue
reticular neurons (for automatic of reflex movements in eating of swallowing) and cortical fibres (for speech articulation)
hypoglossal canal
what is jugular foramen syndrome?
what is it caused by?
what are its symptoms?
what is it caused by?
what are its symptoms?
entrapemnt of any of the last four cranial nerves and or the neraby carotid nerve
tumor (primary form the nasopharynx or secondary from the uper cervical lymph nodes)
symptoms :
- pain in or behind ear due to irritation of the auricular branches of the 9 and 10
- headache due to irritation of the meningeal branch of 10
-hoarseness due to paralysis of the laryngeal nerves
- dysphagia (diffiuclty to swallow) due to paralysis of the pharyngomotor fibres
- honers syndrome ( ptosis of upper eyelid, pupillary constriction) due to interruption of sympathetic internal caortid nerve
- wasting of affected side of tongue and deviation of the protruded tongue to the affected side due to infranuclear paralysis of 12
- deviation of teh uvula away form the affected side due to unoposed action of levator palatini
- sensory loss in oroharynx on the affected side
- inabllity do adduct the voral cord to the midline
- weakness and wasting of sternocleidomastoid and treapezius due to interruption of 11
sympathetic signs may be absend if accessory nerves will be unaffected
tumor (primary form the nasopharynx or secondary from the uper cervical lymph nodes)
symptoms :
- pain in or behind ear due to irritation of the auricular branches of the 9 and 10
- headache due to irritation of the meningeal branch of 10
-hoarseness due to paralysis of the laryngeal nerves
- dysphagia (diffiuclty to swallow) due to paralysis of the pharyngomotor fibres
- honers syndrome ( ptosis of upper eyelid, pupillary constriction) due to interruption of sympathetic internal caortid nerve
- wasting of affected side of tongue and deviation of the protruded tongue to the affected side due to infranuclear paralysis of 12
- deviation of teh uvula away form the affected side due to unoposed action of levator palatini
- sensory loss in oroharynx on the affected side
- inabllity do adduct the voral cord to the midline
- weakness and wasting of sternocleidomastoid and treapezius due to interruption of 11
sympathetic signs may be absend if accessory nerves will be unaffected
what are the six branches the intertal carotid gives off?
1 hypophyseal branch wiithin the cavernous sinus to the neurohypophysis ( pituitary protal system)
2 opthalamic artery ( to orbit though optic cancal) supplies the following structures: - structures in orbit,
- the frontal and ethmoidal sinuses
-frontal scalp
-dorsum of nouse
3 anterior choriodal artery supplies optic tract choroid plexus of the ltateral ventrilce, hippocampus, deep structures of the cerebral hemisohere like the internal capsule and the pallidum
4 posteror communicating artery anastomses then with the posterior cerebral artery and forms the cerebral arterial circle of willis
5 and 6 terminal branches of it are the anterior and middle cerebral arteries
2 opthalamic artery ( to orbit though optic cancal) supplies the following structures: - structures in orbit,
- the frontal and ethmoidal sinuses
-frontal scalp
-dorsum of nouse
3 anterior choriodal artery supplies optic tract choroid plexus of the ltateral ventrilce, hippocampus, deep structures of the cerebral hemisohere like the internal capsule and the pallidum
4 posteror communicating artery anastomses then with the posterior cerebral artery and forms the cerebral arterial circle of willis
5 and 6 terminal branches of it are the anterior and middle cerebral arteries
what are the brances of the vertebral arteries?
anterior and posterior spinal arteries suppplying the medulla and spinal cord
posterior inferior cerebellar artery ( suppplies the inferor aspect of the cerebellum=
as the verteberal arteries merge together, they form the basilar artery which gibes rise to hte anteror inferior cerebllar artery (supplies the anterior and inferior part of hte cerebllum)
pontine branches
superior cerebral arteries (supplying the visual cortex and occpiputal lobe)
posterior inferior cerebellar artery ( suppplies the inferor aspect of the cerebellum=
as the verteberal arteries merge together, they form the basilar artery which gibes rise to hte anteror inferior cerebllar artery (supplies the anterior and inferior part of hte cerebllum)
pontine branches
superior cerebral arteries (supplying the visual cortex and occpiputal lobe)
what other names are there for stroke?
by what is it caused?
what are the associations of a stroke involving the internal carotid system?
vertebrobasilar system?
by what is it caused?
what are the associations of a stroke involving the internal carotid system?
vertebrobasilar system?
cerebrovascular accident (CVA)
ictus cerebri
sudden occlusion of the cerebral artery
rupture of blood vessel (cerebral haemorrhage)
focal epilepsy contrallteral sennsory motor deficit and psychological deficits (aphasia)
focal brainstem syndrome
ictus cerebri
sudden occlusion of the cerebral artery
rupture of blood vessel (cerebral haemorrhage)
focal epilepsy contrallteral sennsory motor deficit and psychological deficits (aphasia)
focal brainstem syndrome


1 anterior cerebral artery
2 middle cerebral artery
3 anterior communicating artery
4 posterior cerebral artery
5 posteror communicating artery
6 internal carotid artery
7 common carotid artery
8 vertebral arteries
9 external carotid artery (not so important)
10 basilar artery
11right middle cerebral artery
12 circle of willis
2 middle cerebral artery
3 anterior communicating artery
4 posterior cerebral artery
5 posteror communicating artery
6 internal carotid artery
7 common carotid artery
8 vertebral arteries
9 external carotid artery (not so important)
10 basilar artery
11right middle cerebral artery
12 circle of willis

A Granule cell (ranule cells refer to tiny neurons (a type of cell) that are around 10 micrometres in diameter. Granule cells are found within the granular layer of the cerebellum, layer 3, inner most layer, of cerebellar cortex. Cerebellar granule cells account for nearly half of the neurons in the central nervous system. Granule cells receive excitatory input from mossy fibers originating from pontine nuclei. Cerebellar granule cells send parallel fibers up through the Purkinje layer into the molecular layer where they branch out and spread through Purkinje cell dendritic arbors. These parallel fibers form thousands of excitatory synapses onto the intermediate and distal dendrites of Purkinje cells using glutamate as a neurotransmitter)
b molecular layer
c purkenje fiber
d granular layer
f white layer
g Climbing fibres from
inferior olivary nucleus
h mossy fiber
b molecular layer
c purkenje fiber
d granular layer
f white layer
g Climbing fibres from
inferior olivary nucleus
h mossy fiber

deep within each cerebral hemisphere lies grey matter known as basal ganglia. they include 7 . name them
the striatum (or neostriatum);
-caudate nucleus
-nucleus accumbens
- putamen
• the pallidum (= globus pallidus)
- lateral segment
- medial segment
• subthalamic nucleus
• pars compacta of substantia nigra
-caudate nucleus
-nucleus accumbens
- putamen
• the pallidum (= globus pallidus)
- lateral segment
- medial segment
• subthalamic nucleus
• pars compacta of substantia nigra

The striatum (caudate and putamen) is often regarded as the input portion of the basal ganglia, since most of the afferent projects into here rather than the pallidum. They originate in three sources. name them and ther fibres and where they originate.
the cerebral cortex
the thalamus
substantia nigra
• Corticostriatal fibres o
• Thalamostriatal fibres o.
• Nigrostriatal fibres
the thalamus
substantia nigra
• Corticostriatal fibres o
• Thalamostriatal fibres o.
• Nigrostriatal fibres
effernt fibres form the striatum projects as medium spiny neurons mainly to three destinations . name them .
the lateral and medial segments of the pallidum (striatopallidal fibres) and the pars reticulata of the substantia nigra (striatonigral fibres). they use gaba as their neurotransmitter which is inhibitory fo the pallidal and nigral neurons.
The two segments of the pallidum receive similar afferent fibres,from two different structures. name them.
striatal GABAergic neurons (as mentioned above), as well as the
subthalamic nucleus (a small diencephalic structure lying beneath the thalamus and against the medial surface of the internal capsule).
subthalamic nucleus (a small diencephalic structure lying beneath the thalamus and against the medial surface of the internal capsule).
efferent fibres of the lateral segment of the pallidum project where? are these ones inhibitory or excitory? whrer do the medial ones travel to? are they inhibitory or excitory?
subthalamic nucleus and subthalamic fasciculus.
inhibitory, GABAergic pallidosubthalamic fibres also travel in the subthalamic
fEfferent fibres of the medial segment, also inhibitory and GABAergic, project principally, along with fibres of the pars reticulata of the substantia nigra, to the thalamus
inhibitory, GABAergic pallidosubthalamic fibres also travel in the subthalamic
fEfferent fibres of the medial segment, also inhibitory and GABAergic, project principally, along with fibres of the pars reticulata of the substantia nigra, to the thalamus

smooth stelate cells receive collateral branches form the pyramidal cells.
can be found in whcih lamina?
are they excitory or inhibitory?
which neurotransmitter do tehy use?
where do they synapse (tip,same as spiny stellate)?
there are classified into three types accodring to their synapse loaction. which are they?
can be found in whcih lamina?
are they excitory or inhibitory?
which neurotransmitter do tehy use?
where do they synapse (tip,same as spiny stellate)?
there are classified into three types accodring to their synapse loaction. which are they?
lamina IV, form inhibitory γ-aminobutyric acid (GABA)ergic synapses on other pyramidal cells.
axodendritic (onto the bases of spines of pyramidal
cell dendrites),
axosomatic (onto the soma of pyramidal cells, also known as basket cells)
and axoaxonal (onto the axons of several pyramidal cells, also known as chandelier cells).
the neocortex (neopallium) isevolutionay recent. it constitues the remaining 90% of the cerebral cortex and is made up of six lamina. name them.
I. Molecular Layer containing tips of apical dendrites of pyramidal cells as well as the most
distal branches of corticothalamic axons of the intralaminar nucleus of the thalamus.
II. Outer Granular Layer containing small pyramidal cells which establish intracortical
connections.
III. Outer Pyramidal Layer containing medium-sized pyramidal cells which give rise to
association and commissural fibres, and stellate cells.
IV. Inner Granular Layer containing stellate cells, especially in the primary somatosensory,
primary visual and primary auditory cortices, and which receive thalamocortical
afferents
V. Inner Pyramidal Layer containing large pyramidal cells projecting to extracortical targets
including the corpus striatum, thalamus, brainstem and spinal cord
VI. Fusiform Layer containing modified pyramidal cells projecting to the thalamus†
distal branches of corticothalamic axons of the intralaminar nucleus of the thalamus.
II. Outer Granular Layer containing small pyramidal cells which establish intracortical
connections.
III. Outer Pyramidal Layer containing medium-sized pyramidal cells which give rise to
association and commissural fibres, and stellate cells.
IV. Inner Granular Layer containing stellate cells, especially in the primary somatosensory,
primary visual and primary auditory cortices, and which receive thalamocortical
afferents
V. Inner Pyramidal Layer containing large pyramidal cells projecting to extracortical targets
including the corpus striatum, thalamus, brainstem and spinal cord
VI. Fusiform Layer containing modified pyramidal cells projecting to the thalamus†
list the 5 afferent (incoming) fibres to the cortex which go to any given region of the cortex. they derive form these 5 sources.
1. Long or short association fibres from small and medium-sized pyramidal cells of the ipsilateral cortex. Long association fibres arise in another lobe, while short association fibres arise much closer, often in a neighbouring gyrus
2. Commissural fibres from medium-sized pyramidal cells projecting mainly through the corpus callosum from matching areas in the contralateral hemisphere.
3. Specific thalamocortical fibres from the appropriate specific or association nucleus (e.g. from the ventral posterior thalamic nucleus → somatosensory cortex; from the dorsomedial thalamic nucleus → prefrontal cortex).
4. Non-specific thalamocortical fibres from the intralaminar nuclei.
5. Cholinergic and aminergic fibres from the basal forebrain, hypothalamus and brainstem.
2. Commissural fibres from medium-sized pyramidal cells projecting mainly through the corpus callosum from matching areas in the contralateral hemisphere.
3. Specific thalamocortical fibres from the appropriate specific or association nucleus (e.g. from the ventral posterior thalamic nucleus → somatosensory cortex; from the dorsomedial thalamic nucleus → prefrontal cortex).
4. Non-specific thalamocortical fibres from the intralaminar nuclei.
5. Cholinergic and aminergic fibres from the basal forebrain, hypothalamus and brainstem.
Pyramidal cells give rise to the only efferents from the cerebral cortex, all of which are excitatory. They often innervate other areas of cortex, and so a proportion has already been
mentioned in the list of afferents (namely, long and short association fibres and commissural fibres)
mentioned in the list of afferents (namely, long and short association fibres and commissural fibres)
1. Short association fibres (e.g. those entering the primary motor cortex from the primary somatosensory cortex) and long association fibres (e.g. those projecting back from the
prefrontal cortex to sensory association areas of the parietal lobe).
2. Commissural fibres running across the corpus callosum, anterior commissure and other minor commissures, to matching areas in the contralateral cortex.
3. Projection fibres, especially
a. corticostriatal (from primary motor and somatosensory cortices to the basal ganglia)
b. corticothalamic (from all areas of cortex to the thalamus)
c. corticopontine (to ipsilateral pontine nuclei)
d. corticonuclear (to contralateral motor and somatic sensory cranial nerve nuclei in the
pons and medulla)
e. corticospinal (to motor neurons of the anterior horn of the spinal cord)
prefrontal cortex to sensory association areas of the parietal lobe).
2. Commissural fibres running across the corpus callosum, anterior commissure and other minor commissures, to matching areas in the contralateral cortex.
3. Projection fibres, especially
a. corticostriatal (from primary motor and somatosensory cortices to the basal ganglia)
b. corticothalamic (from all areas of cortex to the thalamus)
c. corticopontine (to ipsilateral pontine nuclei)
d. corticonuclear (to contralateral motor and somatic sensory cranial nerve nuclei in the
pons and medulla)
e. corticospinal (to motor neurons of the anterior horn of the spinal cord)

what are the main afferent projections to the cerebellum?
where to they termintate?
are they excitory or inhibitory?
what are mossy and climbing fibres?
where to they termintate?
are they excitory or inhibitory?
what are mossy and climbing fibres?
1. spinocerebellar fibres (from the spinal
cord)
2.olivocerebellar fibres (from the inferior olivary nucleus of the medulla oblongata),
3. vestibulocerebellar fibres (from the vestibular nuclei), and 4.pontocerebellar fibres (from the
pons). T
they mostly terminate in the cerebellar cortex where they are excitatory to cortical neurons.
Afferent fibres enter through one of the cerebellar peduncles and proceed to the cortex as either mossy fibres or climbing fibres, depending on their origin (only the olivocerebellar fibres end as climbing fibres). Each mossy fibre branches to supply several folia,
ending in the granular layer in synaptic contact with granule cells.
cord)
2.olivocerebellar fibres (from the inferior olivary nucleus of the medulla oblongata),
3. vestibulocerebellar fibres (from the vestibular nuclei), and 4.pontocerebellar fibres (from the
pons). T
they mostly terminate in the cerebellar cortex where they are excitatory to cortical neurons.
Afferent fibres enter through one of the cerebellar peduncles and proceed to the cortex as either mossy fibres or climbing fibres, depending on their origin (only the olivocerebellar fibres end as climbing fibres). Each mossy fibre branches to supply several folia,
ending in the granular layer in synaptic contact with granule cells.
what fibres does the medal gracile fasciculus carry ?
which fibres does the laterl cuneate fasciculus carry?
which fibres does the laterl cuneate fasciculus carry?
medial gracile fasciculus carrying fibres from the lower trunk and lower
limb, the lateral cuneate fasciculus carrying fibres from the upper trunk and upper limb.
The second order afferents arise in the gracile and cuneate nuclei,
limb, the lateral cuneate fasciculus carrying fibres from the upper trunk and upper limb.
The second order afferents arise in the gracile and cuneate nuclei,
Brainstem Death
Lesions of the brainstem may be caused by stroke, tumour or multiple sclerosis, and can have
serious consequences, including three things.
Lesions of the brainstem may be caused by stroke, tumour or multiple sclerosis, and can have
serious consequences, including three things.
• ipsilateral cranial nerve dysfunction
• contralateral spastic hemiparesis (= paralysis of one side of the body)
• hyperreflexia (= exaggeration of the deep tendon reflexes) and extensor plantar response
• contralateral hemisensory loss
• ipsilateral incoordination
• contralateral spastic hemiparesis (= paralysis of one side of the body)
• hyperreflexia (= exaggeration of the deep tendon reflexes) and extensor plantar response
• contralateral hemisensory loss
• ipsilateral incoordination
what is the cisterna magna
The cisterna magna (or cerebellomedullary cistern) is one of three principal openings in the subarachnoid space between the arachnoid and pia mater layers of the meninges surrounding the brain. The openings are collectively referred to as cisterns. The cisterna magna is located between the cerebellum and the dorsal surface of the medulla oblongata. Cerebrospinal fluid produced in the fourth ventricle drains into the cisterna magna via the lateral apertures and  median aperture.
median aperture.
median aperture.
a thalamus
b superior colliculus
c inferior colliculus
d locus coeruleus is a nucleus in the brain stem involved with physiological responses to stress and panic
e vestibular area (lateral to sulcus limitans)
f vagal trigone
g cuneate tubercle (carrying fine touch and proprioceptive information from the upper body (above T6, excepting the face and ear - the information from the face and ear is carried by the primary sensory trigeminal nucleus) to the thalamus and cerebellum via the medial lemniscus)
h gracile tubercle It contains second-order neurons of the dorsal column-medial lemniscus system, which receive inputs from sensory neurons of the dorsal root ganglia and send axons that synapse in the thalamus.
i obex (The obex (from the Latin for barrier) is the point in the human brain at which the fourth ventricle narrows to become the central canal of the spinal cord.The obex occurs in the caudal medulla. The decussating of sensory fibers happens at this point.)
j hypoglossal trigone
k fascial colliculus The facial colliculus is an elevated area located on the dorsal pons. It is formed by motor fibres of the facial nerve
l inferor
m middle
n suoerior cerebellar peduncles
o trochlear nerve
p pineal gland
q cerebellar peduncles
b superior colliculus
c inferior colliculus
d locus coeruleus is a nucleus in the brain stem involved with physiological responses to stress and panic
e vestibular area (lateral to sulcus limitans)
f vagal trigone
g cuneate tubercle (carrying fine touch and proprioceptive information from the upper body (above T6, excepting the face and ear - the information from the face and ear is carried by the primary sensory trigeminal nucleus) to the thalamus and cerebellum via the medial lemniscus)
h gracile tubercle It contains second-order neurons of the dorsal column-medial lemniscus system, which receive inputs from sensory neurons of the dorsal root ganglia and send axons that synapse in the thalamus.
i obex (The obex (from the Latin for barrier) is the point in the human brain at which the fourth ventricle narrows to become the central canal of the spinal cord.The obex occurs in the caudal medulla. The decussating of sensory fibers happens at this point.)
j hypoglossal trigone
k fascial colliculus The facial colliculus is an elevated area located on the dorsal pons. It is formed by motor fibres of the facial nerve
l inferor
m middle
n suoerior cerebellar peduncles
o trochlear nerve
p pineal gland
q cerebellar peduncles
what is the tegmentum
what is the tectum
what is the tectum
The tectum is a region of the brain, specifically the dorsal part of the mesencephalon (midbrain). T. It is responsible for auditory and visual reflexes.
The tegmentum is a general area within the brainstem. It is located between the ventricular system and distinctive basal or ventral structures at each level. It forms the floor of the midbrain whereas the tectum forms the ceiling.[2] It is a multisynaptic network of neurons that is involved in many unconscious homeostatic and reflexive pathways.

The tegmentum is a general area within the brainstem. It is located between the ventricular system and distinctive basal or ventral structures at each level. It forms the floor of the midbrain whereas the tectum forms the ceiling.[2] It is a multisynaptic network of neurons that is involved in many unconscious homeostatic and reflexive pathways.


what does the paleocerebellum consist of
what does it influence
which fibres terminate in it
what does it influence
which fibres terminate in it
consists of the vermis and adjacent parts of the cerebellar hemispheres - the paravermis, within both the anterior and posterior lobes.
influences muscle tone and posture.
Afferent fibres from muscle, joint and cutaneous receptors terminate in the ipsilateral paleocerebellum through the inferior and superior cerebellar peduncles.
influences muscle tone and posture.
Afferent fibres from muscle, joint and cutaneous receptors terminate in the ipsilateral paleocerebellum through the inferior and superior cerebellar peduncles.
what does the ventral spinocerebellar tract? where does t cross over?
proprioceptive information from the body to the cerebellum. It is part of the somatosensory system and runs in parallel with the dorsal spinocerebellar tract. Both these tracts involve two neurons. The ventral spinocerebellar tract will cross to the opposite side of the body then cross again to end in the cerebellum (referred to as a "double cross"), as compared to the dorsal spinocerebellar tract, which does not decussate, or cross sides, at all through its path.
what is the globose nucleus?
whcih fibres pass through it ( and the embolifrom as well)
whcih fibres pass through it ( and the embolifrom as well)
The globose nucleus is one of the deep cerebellar nuclei. It is located medial to the emboliform nucleus and lateral to the fastigial nucleus. This nucleus contains primarily large and small multipolar neurons.
Efferents pass to the deep nuclei of the cerebellum (especially the globose and emboliform), which project in turn via the superior cerebellar peduncle to the contralateral red nucleus of the
midbrain and influence the descending rubrospinal tract
Efferents pass to the deep nuclei of the cerebellum (especially the globose and emboliform), which project in turn via the superior cerebellar peduncle to the contralateral red nucleus of the
midbrain and influence the descending rubrospinal tract
what are pontocerebellar fibres?
by what regions are the influenced by?
by what regions are the influenced by?
afferent pathway in neocerebellum consists of pontocerebellar fibres, i.e. neurons originating in the pontine nuclei of the basal portion of the pons projecting across the midline to enter the contralateral
cerebellar hemisphere through the middle cerebellar peduncle. The pontocerebellar neurons
are influenced by widespread regions of the cerebral cortex involved in the planning and execution of movements.
The pontocerebellar neurons themselves project predominantly to the
l
cerebellar hemisphere through the middle cerebellar peduncle. The pontocerebellar neurons
are influenced by widespread regions of the cerebral cortex involved in the planning and execution of movements.
The pontocerebellar neurons themselves project predominantly to the
l
the ventral lateral nucleus of the thalamus projects to which structure? what does that indicate ( think of the neocerebellum)
cerebral cortex, particularly the motor cortex of the frontal lobe.
In this way the neocerebellum exerts a coordinating role in movement by on the motor cortex and its descending corticospinal and corticobulbar pathways.
In this way the neocerebellum exerts a coordinating role in movement by on the motor cortex and its descending corticospinal and corticobulbar pathways.
what is the arnold chiari malformation
how does it present in children
how does it present in children
congenital or acquired condition where the cerebellar tonsils are forced through the foramen magnum, often blocking
the flow of CSF and compressing or stretching the brainstem, lower cranial nerves or inferior
Infants may present with stridor (a high pitched sound of turbulent gas flow in the upper respiratory tract) and swallowing difficulties, older children with upper and progressive lower limb weakness and breathing difficulties.
the flow of CSF and compressing or stretching the brainstem, lower cranial nerves or inferior
Infants may present with stridor (a high pitched sound of turbulent gas flow in the upper respiratory tract) and swallowing difficulties, older children with upper and progressive lower limb weakness and breathing difficulties.
what does the cerebellum consist of? think of cortexes and nuclei
outer cortex of grey matter, and an inner core of afferent and efferent white matter, the branching projections of which form a tree like pattern – the so-called arbor vitae. Deep within the white matter are buried four pairs of cerebellar nuclei, from medial to lateral;
1. dentate nucleus (with a serrated or toothed appearance in section); the only deep
nucleus easily visible to the naked eye),
2. globose nucleus )
3. emboliform nucleus
4. fastigial nucleus considered part of the archicerebellum.
The globose and emboliform nuclei, lying between the dentate and fastigial, are sometimes
collectively referred to as the interposed nuclei.
1. dentate nucleus (with a serrated or toothed appearance in section); the only deep
nucleus easily visible to the naked eye),
2. globose nucleus )
3. emboliform nucleus
4. fastigial nucleus considered part of the archicerebellum.
The globose and emboliform nuclei, lying between the dentate and fastigial, are sometimes
collectively referred to as the interposed nuclei.

a mammary body
b optic tract
c interpedencular fossa
d cerebral peducle
e pons
f pyramid
g loive
h decussation of pyramids
i spinal cord
j spinal acessory nerve (11)
k cranial accesory nerve (11)
l vagus nerve 10
m hypoglossal nerve 12
n glosopharyngeal nerve 9
o vestibuloochlear 8
p nervus intermedius
q facial nerve 7
r abducens (6)
s sensory root
t motor root
u trigeminral nerve
v trochlear nerve 4
w oculomotor nerve 3
x infundibulum
y optic nerve 2
b optic tract
c interpedencular fossa
d cerebral peducle
e pons
f pyramid
g loive
h decussation of pyramids
i spinal cord
j spinal acessory nerve (11)
k cranial accesory nerve (11)
l vagus nerve 10
m hypoglossal nerve 12
n glosopharyngeal nerve 9
o vestibuloochlear 8
p nervus intermedius
q facial nerve 7
r abducens (6)
s sensory root
t motor root
u trigeminral nerve
v trochlear nerve 4
w oculomotor nerve 3
x infundibulum
y optic nerve 2


A premotor cortex
B precentral gyros primary motor cortex
C central sulcus
D postcentral gyros somatosensory cortex
E superior parietal lobule
F intraparietal sulcus
G inferior parietal sulcus
H primary virual center
I auditory associaton cortex (wenickes area)
J primary auditory cetner
K superior temporl gyros
L lateral frissure
M borcas area
N frontal eye field
B precentral gyros primary motor cortex
C central sulcus
D postcentral gyros somatosensory cortex
E superior parietal lobule
F intraparietal sulcus
G inferior parietal sulcus
H primary virual center
I auditory associaton cortex (wenickes area)
J primary auditory cetner
K superior temporl gyros
L lateral frissure
M borcas area
N frontal eye field

whre to afferent fibres to primary motor cortex originate from?
where does that origin receive its input from ?
where does that origin receive its input from ?
Afferent (incoming) fibres to the primary motor cortex originate principally from the thalamus (the ventral lateral nucleus), which in turn receives input from the dentate nucleus of the
cerebellum and the pallidum of
the basal ganglia.
cerebellum and the pallidum of
the basal ganglia.
what kind of afferent fibres does the premotor cortex receive and where do they come from? with what fibres is the premotor cortex in contact with the primary motor cortex?
premotor cortex has short association fibres with which it communicates with the primary motor cortex
afferent fibres to the premotor cortex form the thalamus (ventral anterior nucleus), which in turn receives fibres from the globus pallidus of the basal ganglia and the
substantia nigra of the midbrain.
afferent fibres to the premotor cortex form the thalamus (ventral anterior nucleus), which in turn receives fibres from the globus pallidus of the basal ganglia and the
substantia nigra of the midbrain.
what kiind of fibres does the prefrontal lobe have?
where do they origintae?
what it the lobe involved in
where do they origintae?
what it the lobe involved in
long association (i.e. interlobar)
fibres
Afferent fibres originate principally in the thalamus (mediodorsal and anterior nuclei
It
is involved in cognition, including faculties of intellect, judgement, prediction and the
planning of behaviour.
fibres
Afferent fibres originate principally in the thalamus (mediodorsal and anterior nuclei
It
is involved in cognition, including faculties of intellect, judgement, prediction and the
planning of behaviour.
lesions of the dominant left frontal lobe can cause three things. list them.
• Paroxysmal (i.e. short, frequent) jerking movements in a contralateral limb, known as simple motor or Jacksonian seizures
• contralateral hemiplegia, with weakness of the face and upper motor neuron signs in the limb
• Broca's aphasia with difficulty producing brief utterances, paraphasia (word errors) and poor
articulation. Word repetition is impaired, but comprehension preserved. Alexia and agraphia
(complete inability to read or write) may present.
the ventral posterior nucleus (thalamus) receives fibres form where? (three parts=
- the medial lemniscus - a
brainstem pathway for second order afferent neurons
(conveying information about fine touch and proprioception)
• the spinal lemniscus (coarse touch and pressure) and
spinothalamic tracts (pain and temperature)
• trigeminothalamic tracts (general sensation from the head)
brainstem pathway for second order afferent neurons
(conveying information about fine touch and proprioception)
• the spinal lemniscus (coarse touch and pressure) and
spinothalamic tracts (pain and temperature)
• trigeminothalamic tracts (general sensation from the head)
lesions to the left parietal lobe may cause what? (three points)?
• paroxysmal attacks of abnormal sensations spreading down the contralateral side of the body (sensory seizures)
• a contralateral hemisensory loss (i.e. loss of feeling on the opposite side of the body) and inferior
visual field loss
• inability to name objects, read, write and/or calculate (technically known as anomia, alexia, agraphia and acalculia, respectively)
• a contralateral hemisensory loss (i.e. loss of feeling on the opposite side of the body) and inferior
visual field loss
• inability to name objects, read, write and/or calculate (technically known as anomia, alexia, agraphia and acalculia, respectively)
lesions to the right parietal lobe may cause three things?
• paroxysmal attacks of sensory disturbance affecting the contralateral side of the body (simple
sensory seizures)
• a contralateral hemisensory loss and inferior visual field loss
• spatial disorientation resulting in an inability to copy and construct designs (constructional
apraxia)
sensory seizures)
• a contralateral hemisensory loss and inferior visual field loss
• spatial disorientation resulting in an inability to copy and construct designs (constructional
apraxia)
the primary auditory cortex is located at the superior part of the temporal gyros within the lateral firssure. it is marked by a transerve temporal gyri. for what is it responsible?
which fibres does it receive?
which fibres does it receive?
-conscious perception of sound, different wavelengths of which are
perceived tonotopically within the cochlear duct. The primary auditory
- afferent fibres from the thalamus (the medial geniculate nucleus), which in turn receives ascending acoustic fibres that have undergone partial decussation (crossing-over) in the brainstem. This
means that acoustic sensation from both ears is represented in each primary auditory cortex,
perceived tonotopically within the cochlear duct. The primary auditory
- afferent fibres from the thalamus (the medial geniculate nucleus), which in turn receives ascending acoustic fibres that have undergone partial decussation (crossing-over) in the brainstem. This
means that acoustic sensation from both ears is represented in each primary auditory cortex,
in the dominant hemisphere the auditory association cortex is known as what and is necessary for what?
Wernicke's area, which is necessary for understanding of the spoken word and has i connections with other language areas of the brain (e.g. with Broca's area by the long association fibres of the arcuate fasciculus
associated with the cochlear is a structures. it runs with the cochlear neruce as the 8th cranical nerve (vestibulocochlear nerve). name them and what they are resonsible for.
semicircular canals of the vestibular system responsible for the sense of balance. The vestibular nerve runs with the cochlear nerve
as the VIIIth cranial (vestibulocochlear) nerve
as the VIIIth cranial (vestibulocochlear) nerve
the inferomedial part of the temporal lobe is curled in on itself and forms what? it is associated with what sturcutre? to which system does it belong? what are its funtion?
hippocampus
ssociated with the floor lateral ventricle, deep to the
parahippocampal gyrus
It forms part of the limbic system
associated with long term memory and the emotional aspects of behaviour.
ssociated with the floor lateral ventricle, deep to the
parahippocampal gyrus
It forms part of the limbic system
associated with long term memory and the emotional aspects of behaviour.
where is the amygdala situated?
to what system does it belong?
what type of matter is it?
what structures does ut recieve?
to what system does it belong?
what type of matter is it?
what structures does ut recieve?
Near the anterior end of the hippocampus and the anterior end of the lobe (the temporal pole),
grey matter
limbic system
fibres from the olfactory tract (Ist cranial nerve),
and are involved in the conscious appreciation of the sense of smell.
grey matter
limbic system
fibres from the olfactory tract (Ist cranial nerve),
and are involved in the conscious appreciation of the sense of smell.
lesions of the dominant temporal lobe may cause what? three things
• paroxysmal attacks of unresponsiveness (absences), purposeless behaviour (automatism), olfactory, visual and/or auditory hallucinations, and disturbances of mood
and memory (déjà vu)(complex partial seizures)
• contralateral superior visual field loss
• rapid, fluent speech rendered incomprehensible by word errors (paraphasia). Profound word finding difficulty, impaired repetition of words and profound loss of comprehension (Wernicke’s aphasia)
and memory (déjà vu)(complex partial seizures)
• contralateral superior visual field loss
• rapid, fluent speech rendered incomprehensible by word errors (paraphasia). Profound word finding difficulty, impaired repetition of words and profound loss of comprehension (Wernicke’s aphasia)
with what is the remainder of the occipital cortex (assocation cortex) concerned? what does unilateral damage cause the primary visual cortex? what does damage to the visual assocaition cortex create?
interpretation of images
Unilateral damage to the primary visual cortex causes blindness in the contralateral visual field,
damage to the visual association cortex creates problems with
recognition and interpretation of images.
lesions of the occipital lobe may cause four things
• paroxysmal visual hallucinations of a simple, unformed nature, e.g. lights or colours
• contralateral visual field loss (contralateral homonymous hemianopia)
- Rare bilateral lesions of the occipital lobe (due to stroke or head injury) may lead to cortical blindness of which the patient is unaware (Anton’s blindness or Anton-Babinski syndrome)
-Bilateral parietooccipital lesions may spare elementary vision, but prevent the recognition or depiction of objects
(apperceptive visual agnosia).
• contralateral visual field loss (contralateral homonymous hemianopia)
- Rare bilateral lesions of the occipital lobe (due to stroke or head injury) may lead to cortical blindness of which the patient is unaware (Anton’s blindness or Anton-Babinski syndrome)
-Bilateral parietooccipital lesions may spare elementary vision, but prevent the recognition or depiction of objects
(apperceptive visual agnosia).
what is white matter and grey matter?
The part of the brain that contains myelinated nerve fibers. The white matter is white because it is the color of myelin, the insulation covering the nerve fibers. The white matter is as opposed to the gray matter (the cortex of the brain which contains nerve cell bodies).
what does the thalamus? What kind of fibres does it contain?
Its function includes relaying sensation, special sense and motor signals to the cerebral cortex, along with the regulation of consciousness, sleep and alertness. The thalamus surrounds the third ventricle. It is the main product of the embryonic diencephalon.



Flashcard set info:
Author: Schnuschnax
Main topic: Medicine
Topic: Anatomy
Published: 17.02.2010
Card tags:
All cards (131)
no tags
